Address
Acıbadem Atasehir Hospital
Atatürk Mah. Turgut Özal Bulvarı A Blok, No:11 Atasehir / İstanbul / Turkiye
Salivary glands are organs or structures located in our head and neck region that produce a digestive aid secretion (saliva) and drain it into connected channels in the mouth, throat, pharynx, nose, sinuses, and other areas.
We have six major salivary glands, three on each side of our face, as well as hundreds of minor (microscopic) salivary glands scattered throughout the mucous membrane. The secretion they produce not only aids in digestion but also provides the necessary moisture for the mouth, throat, nose, and laryngeal cavities.
Below, you can find general information about salivary gland tumors and cancers, as well as detailed information about surgery and the postoperative process.
Please feel free to contact me for more information on salivary gland tumors and cancers.
Best regards,
Prof. Cetin Vural, M.D.
ENT & Head and Neck Surgery Specialist
Salivary glands are organs or structures located in our head and neck region that produce a special secretion called saliva, which is then drained into various areas such as the mouth, throat, pharynx, nose, and sinuses through specific ducts.
There are six major (large) salivary glands, three on each side of our face, as well as hundreds of minor (microscopic) salivary glands scattered throughout the mucous membranes. The secretions produced by these glands not only aid in digestion but also provide the necessary moisture and lubrication for the mouth, throat, nasal cavity, and laryngeal spaces, and serve as a defense mechanism against microorganisms that can cause infections.
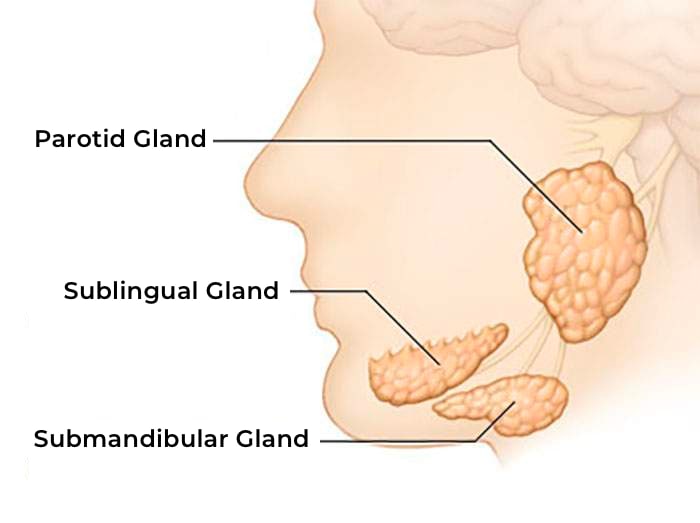
The major salivary glands include:
The parotid salivary glands are structures that extend from the front of our earlobes down to the back of the jawline on both sides of our face. The most important detail about these glands is that the facial nerve, which enables us to make facial expressions, passes through the parotid salivary glands.
The facial nerve travels through the bone of the ear and exits the skull through the mastoid process (a bony protrusion just below the ear) before entering the parotid salivary gland to distribute its branches to the facial muscles.
The parotid gland is divided into two anatomical parts in relation to the facial nerve. The part that lies beneath the skin surface and contains the salivary gland is called the superficial lobe of the parotid. The part that lies deeper in the back of the jawbone is called the deep lobe of the parotid.
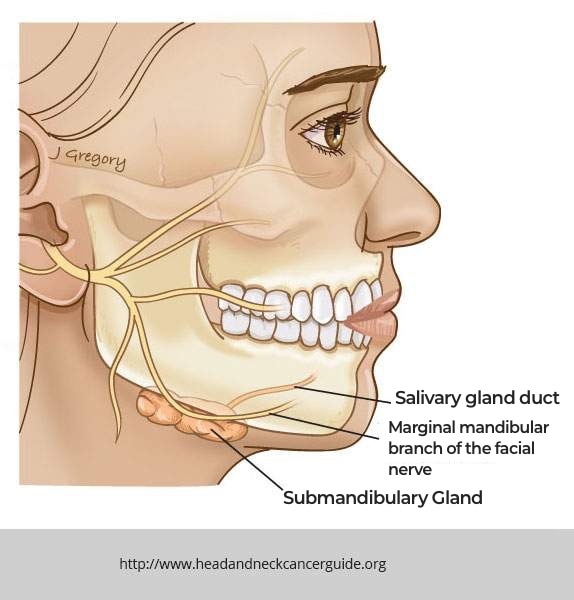

This gland is located under the chin on both sides of our jaw and is the second-largest salivary gland after the parotid gland. Its salivary ducts open on both sides of the floor of our mouth just behind our lower front teeth, near the middle line. The marginal mandibular nerve, which is a branch of the facial nerve, passes over the surface of this gland’s capsule.
Sublingual salivary gland:
Named after the term “sublingual,” which means “under the tongue,” this gland is located under and behind the tongue on both sides. This gland, which empties its saliva into the mouth through multiple ducts, is much less likely to develop tumors compared to the parotid and submandibular glands.
Minor salivary glands:
The covering layer of areas such as the mouth, throat, pharynx, and larynx is called mucosa. To keep this mucosa moist, hundreds of microscopic structures, called minor salivary glands, are located in these areas, invisible to the naked eye. These glands produce saliva 24 hours a day and empty it into these spaces, preventing drying of the mucosal surfaces.

The term “tumor” in Latin means swelling, and it is a term used in medicine to refer to masses that arise from the uncontrolled growth of cells. While any tissue in the body can develop a tumor, salivary glands can also be affected. Tumors can be classified as either benign or malignant. Benign tumors grow more slowly and do not metastasize (spread) to nearby or distant organs. They are usually encapsulated by a thin, membranous covering and do not invade surrounding tissues. They tend to push neighboring tissues aside as they grow, and this growth occurs over months or even years. Benign tumors rarely cause pain, and patients seldom complain of discomfort. If pain is present, it is usually due to indirect causes rather than the tumor itself.
Malignant tumors, on the other hand, grow more rapidly and have the potential to metastasize to nearby lymph nodes and distant organs such as the lungs, liver, brain, and bones. They invade surrounding tissues and disrupt their functions. For example, when they come into contact with neighboring nerves, they can begin to impair their function. Additionally, malignant tumors can cause pain once they reach a certain size. This pain may be due to invasion of structures such as bone or the temporomandibular joint, or it may be caused by direct involvement of nerves that transmit pain signals in the head and face.
In summary, salivary gland tumors;

Salivary gland tumors are most commonly found in the parotid gland. Rarely, tumors can also develop in the submandibular gland, and even more rarely in the sublingual glands. Additionally, tumors can develop in areas where minor salivary glands are located, such as the nasal cavity, sinuses, mouth, throat, pharynx, larynx, and the deep regions of the neck known as the parapharyngeal space.
For example, a biopsy taken from a mass in an area like the nose, palate, or base of the tongue may be reported by a pathology specialist as a tumor originating from the salivary gland. In this case, it is thought that the tumor most likely arises from microscopic salivary glands within the lining tissue, also known as the mucosa.

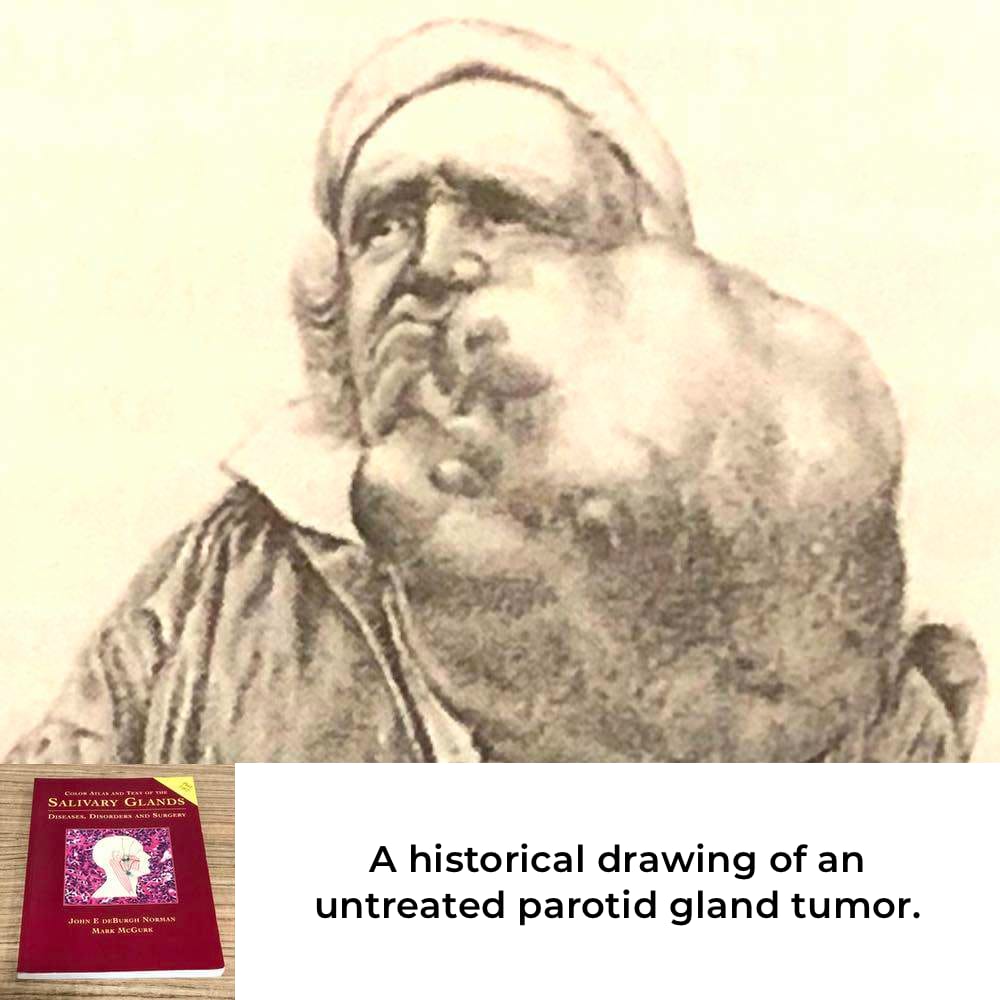
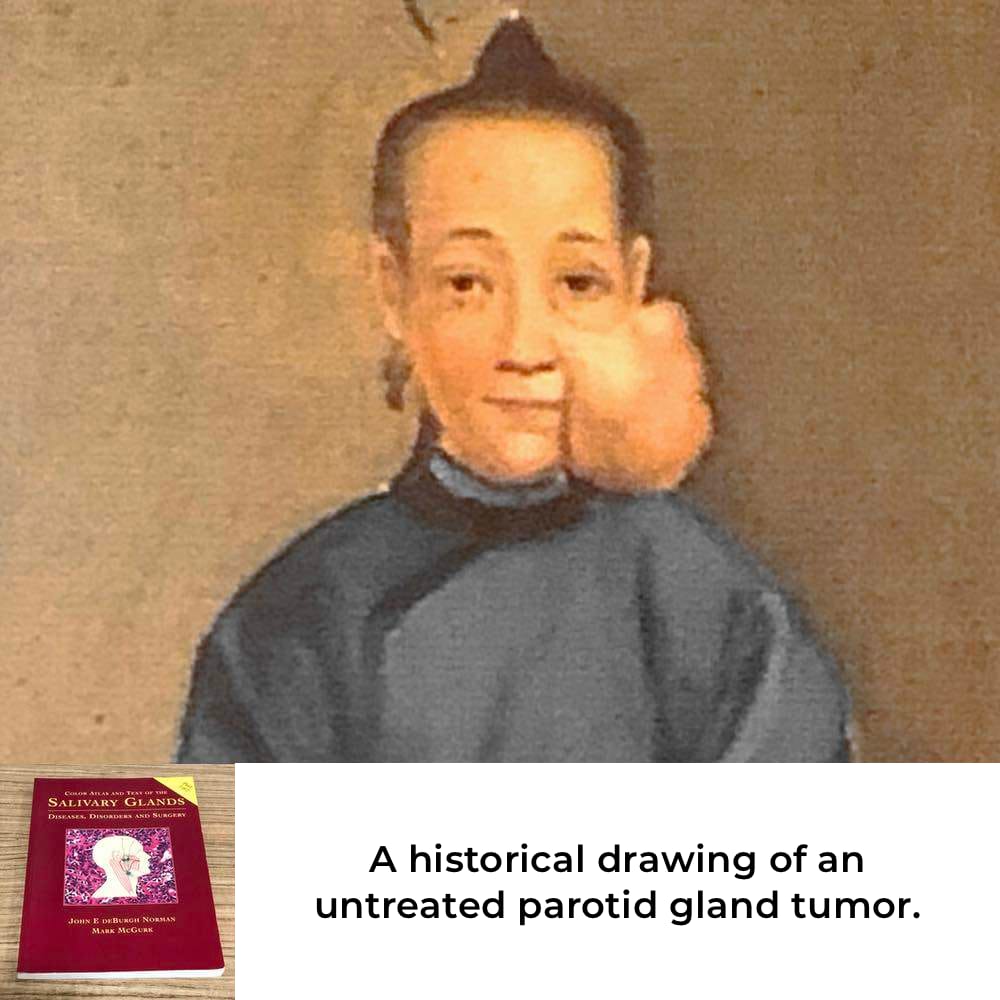
As mentioned above, most salivary gland tumors arise from the parotid gland, especially from the superficial lobe. Rarely, tumors can develop in the deep lobe of the gland. Tumors that arise in the deep lobe are harder to detect and usually appear as a hard lump under the earlobe and behind the lower jaw bone, as compared to tumors that arise in the superficial lobe.
Under this category, some common benign and malignant salivary gland tumors are briefly described.
If left untreated, this tumor carries the risk of transforming into a malignant tumor over the years, a condition known as ‘Carcinoma Ex Pleomorphic Adenoma,’ in which a long-existing, slowly growing mass undergoes a change in behavior and rapidly starts to grow.

MRI image of a benign tumor in the right parotid salivary gland.

MRI image of a benign tumor in the left submandibular salivary gland.
Additionally, the presence of HER2 and Androgen Receptor positivity in the tumor cells, identified through specific pathological staining techniques, may indicate the consideration of targeted therapies in addition to surgery, radiotherapy, and chemotherapy.

Image of our patient’s pleomorphic adenoma that has transformed into salivary gland ductal cancer over a period of 35 years.

MRI images of our patient with carcinoma ex pleomorphic adenoma.

Tomography image of our patient with a tumor in parotid gland.

Cancer is a term used in medicine to describe certain malignant tumors. By definition, there is no such thing as a benign cancer. However, many types of cancer can be completely treated with modern treatment methods. Tumor, on the other hand, is a broader term that encompasses both benign and malignant growths.
If we emphasize the differences:
Benign tumors grow more slowly. They do not metastasize (spread) to nearby or distant organs. They do not invade surrounding tissues. They typically grow by pushing aside the surrounding tissues to make space for themselves. This growth occurs over months or even years. Benign tumors rarely cause pain, and patients rarely complain of pain. If there is pain, it is usually due to indirect reasons rather than the tumor itself.
Malignant tumors (also called malignant or cancerous) grow more rapidly and have the potential to metastasize to regional lymph nodes and distant organs such as the lungs, liver, brain, or bones. They invade surrounding tissues and develop by disrupting their functions. For example, when they reach adjacent nerves, they begin to affect their functions. For instance, if they invade the facial nerve, they can cause facial paralysis.
Furthermore, malignant tumors can cause pain once they reach a certain size. This pain can be due to the invasion of structures such as bones or the temporomandibular joint, or it can directly affect the nerves responsible for sensitivity and pain in the head and facial area.
Benign Tumor:
A typical benign salivary gland tumor is characterized by a slowly growing, painless, rubbery mass that has been noticed by the patient for a long period of time. It can be felt as a movable lump between two fingers. These masses can occur in various areas such as the parotid gland, submandibular gland, or palate.
On magnetic resonance imaging (MRI) or computed tomography (CT) scans, benign tumors appear well-defined and do not show invasive features into surrounding tissues. There are no associated symptoms such as facial paralysis, redness or hardness of the skin over the tumor, swelling or enlargement of lymph nodes in the neck.
During surgery, benign tumors are often observed to have well-defined borders, without extending into the surrounding salivary gland or other tissues. They are encapsulated by a thin membrane called a capsule.
Malignant Tumor:
In contrast, malignant tumors are typically characterized by a more rapid development, growing over weeks or months. They can be painful and feel harder, making it more difficult to move between fingers. On magnetic resonance imaging (MRI) or computed tomography (CT) scans, they often appear infiltrative, invading the surrounding tissues, and their boundaries may not be well-defined.
If they are located near the facial nerve, they can cause facial paralysis by impinging on the nerve. If they are close to the skin, they can result in redness, ulceration, or even the formation of sores. When they spread to the lymph nodes in the neck, they can cause swelling on the sides of the neck.
Advanced tumors in the facial and head-neck region can lead to functional impairments in chewing, swallowing, eating, speaking, and other functions.
During surgery, malignant tumors are often observed to be harder than benign tumors, exhibiting invasion into the surrounding tissues, and they may lack a well-defined capsule surrounding them.
Especially in the development of malignant salivary gland tumors, smoking, alcohol consumption, and exposure to radiation have been implicated as potential factors. However, clear scientific evidence to support these associations has not been established. The causes of benign tumors are even more uncertain.
Salivary gland tumors can occur at any age and in both genders, including childhood. However, benign tumors, such as pleomorphic adenomas, are more commonly observed in the young and middle-aged population, while malignant tumors are more frequently seen in older individuals. There is no significant difference in tumor frequency between males and females.

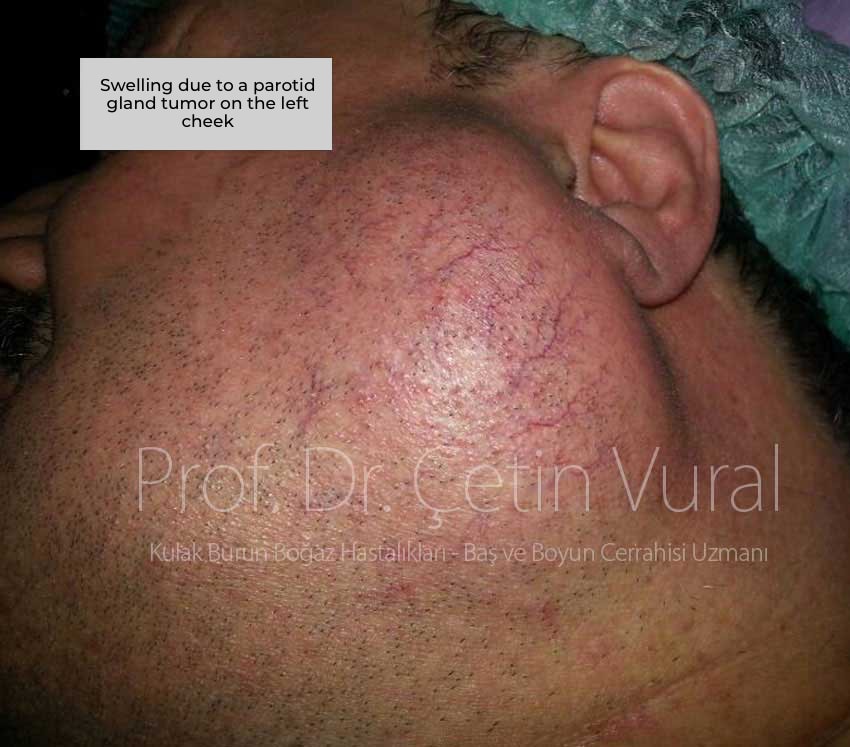
The parotid gland is a gland located in front of and below the ear. Its tumors manifest in this area as swelling, masses, and growth. Typically, they present as a long-standing mass or growth in front of the ear or beneath the earlobe.
This mass often easily moves when pressed between two fingers. The tumor’s growth is usually slow. If the patient delays surgery, the growth of the tumor will become more noticeable over months or years. Tumors originating from the deep lobe may appear as harder-to-detect masses behind the jawbone. Occasionally, they are incidentally discovered on imaging tests such as MRI or CT scans performed for other reasons.
If the tumor is malignant, in addition to swelling, it can be accompanied by pain, facial paralysis, changes in the skin over the tumor surface, ulceration, and swelling of the lymph nodes in the lower parts of the neck.
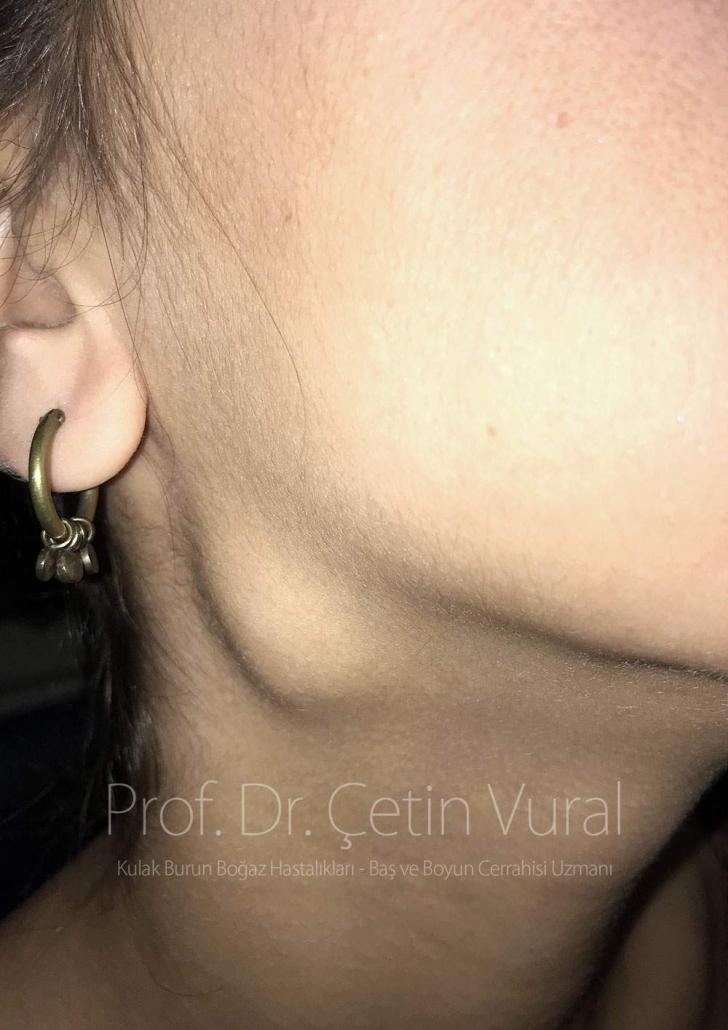
The submandibular salivary gland is an organ located under the jaw. Tumors of this gland may present as swelling beneath the jawbone. Most of these tumors are benign and exhibit slow, painless growth. Typically, there is a mass that has been present for months or even years. In the case of benign tumors, growth is usually very slow after the patient becomes aware of the mass.
If the tumor is malignant (salivary gland cancer), it may be firmer and more pronounced compared to benign tumors. Pain can occur due to involvement of surrounding tissues. Over time, changes in the skin covering the tumor may also be observed. If the tumor adheres to the jawbone, it becomes harder and immobile.
Unlike the parotid gland, submandibular gland stones that obstruct the duct are more commonly seen and can cause intermittent swelling, redness, and pain that resolve afterwards. These stones can sometimes lead to salivary gland infection. In such cases, swelling, pain, and redness increase. Antibiotic treatment and the eventual displacement of the stone can provide relief in these findings. In contrast, swelling associated with tumors does not regress or diminish; it progresses and spreads over time. When encountering such swelling, it is advisable to consult an otolaryngologist and allow them to differentiate between the conditions.

It is highly unlikely for benign parotid tumors (such as pleomorphic adenoma) to cause facial paralysis. However, malignant tumors, as they progress, can invade (disrupt the integrity) the facial nerve that passes through the parotid gland, leading to facial paralysis.


When a suspicion of salivary gland tumor arises, the physician first carefully listens to the patient’s complaints, asks various questions to identify possible accompanying symptoms, and investigates whether there are any notable features related to this condition in the patient’s medical history or family. Subsequently, the examination phase is initiated.
Otorhinolaryngologists generally perform a comprehensive examination of the ear, nose, oral cavity, pharynx, and head and neck, regardless of the reason for the patient’s visit. The tumor is carefully examined through palpation, assessing its size, hardness, mobility, and adherence to surrounding tissues. If the tumor is located in areas such as the nose, mouth, throat, or pharynx, an endoscope, an optical instrument, is used for examination. During these examinations, the presence of enlarged lymph nodes in the neck, decreased facial muscle movement, and weakness are assessed.
Following the physical examination, radiological investigations are performed. Ultrasonography, being the most accessible imaging method, is often the initial choice. The appearance of the mass on the ultrasound is evaluated by the radiologist. Additionally, MRI (magnetic resonance imaging) and CT (computed tomography) provide detailed images, allowing the Otorhinolaryngologist to examine various characteristics related to the tumor in detail.